
Only in the last day or two have COVID test positivity rates started to exceed the rise in testing. The increased testing has already therefore grossly exaggerated Omicron’s effect, and will inevitably do so more as testing mania escalates. But the emphasis on “cases” by the Whittys of this world, the media and most of the public shows that even this elementary bias is not understood, even two years into COVID. Science truly died – together with public understanding – in 2020.
This observation, together with a perceptive article by Sarah Knapton in the Telegraph today, makes it a timely moment to review the distortions built into those old, and never revised, definitions in the ONS data. Casual readers may never have realised the problems, and even regulars may have been bludgeoned by the relentless propaganda to forget!
Knapton’s article, briefly summarised, says this. The South African experience suggests that Omicron is indeed highly contagious, evades many vaccinated people’s immunity, and even that of a good number of those previously infected. At the same time, it is actually very benign – though that may be hard to establish given our official methodology, as I’ll show.
Remember that the sole official definition of a COVID cases is a single positive PCR or LFT test – even if another test is negative. In reply to Sir Desmond Swain in the the Commons debate, Sajid Javid blandly stated that asymptomatic cases are “infected by definition.” He’s right, but the definition itself is meaningless. Furthermore, a COVID death is defined as a death after a positive test within 28 days, with no reference whatsoever to any clinical sign of COVID.
Knapton points out that every January we can expect 0.09% of the population to die naturally, according to the ONS. That, given the misdiagnosis problem, means that if, as predicted by the UKHSA, one million of us have become infected with Omicron by the end of the year, 900+ “cases” will die from the usual causes and be misattributed to Omicron this month. Knapton goes on to use the further estimate of 34.2m Omicron infections by April to show that 30,000 of those, dying from all the usual causes, would be misattributed to COVID. That is a lot of errors.
To put this another way, even if Omicron is so benign that it is incapable of inflicting death, our ONS statistics will inexorably reveal the Armageddon that those like Dr Whitty project. By definition.
Now, Whitty and the other “expert advisers” ought to be fully aware of this, and for the sake of truth and public reassurance at least make reference to it in their pronouncements, even if they don’t alter the whole basis of collecting statistics, which should have been done last year. That said, reading Scott Atlas’s book, it is clear that even close up, those like Drs Fauci and Birx, heading the US Task Force, either didn’t comprehend this simple issue, or had no regard to truth at all. Frighteningly, therefore, SAGE professional incompetence remains a real possibility, the alternative being malice. The only absolute impossibility is that the figures tell the truth. The fact that most of our friends, relatives and journalists accuse sceptics mockingly of “contradicting the top scientists in Britain” proves that rational thought comes hard to the non-experts as well.
Already, then, looking at ONS COVID deaths is meaningless, and will be increasingly so as Omicron replaces Delta and, in all likelihood, sweeps mildly through the population. But the government is only committed to looking at “COVID deaths,” making lockdowns and all that stuff inevitable – probably by January 5th. Lo, I have told you…
We must not forget, of course, that there is, and has since last year, been a strong element of testing casedemic within all the ONS figures. Scott Atlas, in one of his sparse references to UK practice, points out that the UK’S PCR positive rate has been set at 45 cycles – whereas probably anything above 25 indicates no infective virus. 45 cycles doesn’t even over-represent old viral fragments, but many people never even exposed to the virus at all.
This means that at every stage of the pandemic, apart from the initial wave when clinical diagnosis prevailed and testing had not got established, a majority of “cases” have been false positives, and between waves nearly all of them have. This has been confirmed both by theoretical statistics using government false-positive figures, and by careful analysis of the ONS data itself.
This means that from the ONS stats we know almost nothing about the actual prevalence of the disease that we couldn’t discover from sheep entrails. Even hospitalisations and deaths will have been labelled on the basis of false positive tests. Obviously, this exaggeration of cases too will feed into the next few months’ Armageddon figures along with the definitional inaccuracies.
An additional factor (how many more can there be?) is that the “specific test” for Omicron is simply the same old inaccurate PCR test made even more inaccurate by excluding one of the three RNA sequence targets from consideration, since it is absent in the Omicron strain. Previously, its absence would have rendered the test negative: now it diagnoses Omicron. Given what we know of the variant, this does not mean that Omicron is not rampant, but it does mean that the massive testing of the well will rope in all kinds of extra people who have no COVID on board at all.
So we ought to ignore the ONS data altogether if we want to gain any sense of what’s going on, and return to the old epidemiological standard of “excess deaths,” as was advised by proper epidemiologists at the very beginning of the pandemic, but largely ignored by SAGE. But herein there is also a new problem, shown in this latest ONS chart:
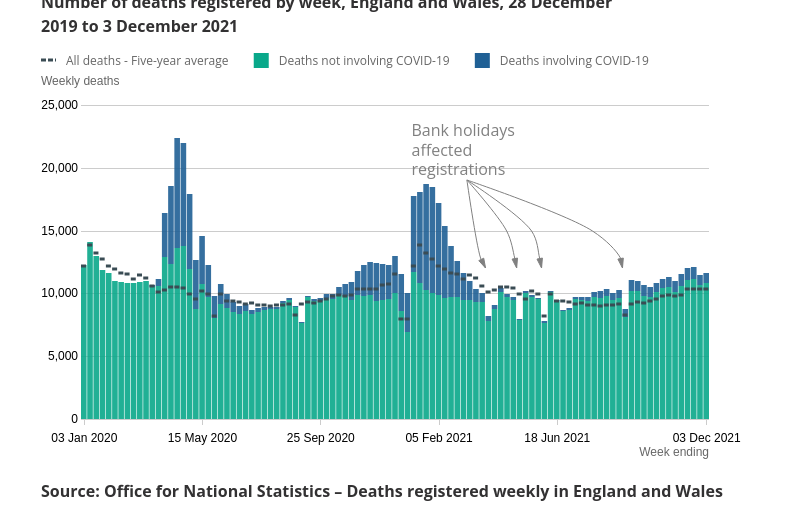
You can see that since early July, Britain has been significantly into the excess death region, even discounting COVID deaths, many of which, as I have shown, have been misattributed because of the amateurish methodology of diagnosis. It does not take a genius to conclude that this excess can only be due due to the measures taken against COVID, including the meltdown of NHS care. That, after all, is not only the subject of many headlines, but was predicted before the first lockdown by me, and even before COVID in the abandoned WHO pandemic plans.
Worse than that, though, the rise post-dates the worst restrictions of lockdown. There is no plausible reason to attribute it to the relaxation of restrictions: but it might very plausibly be related to the roll-out of vaccinations across the age groups not normally contributing to excess deaths, especially children. And booster rollout, of course. That would be worrying if we didn’t know that vaccines are safe and effective in all ages, at all doses, because we have been told so by the country’s leading scientists (after dissenters were removed from the JCVI).
But on the subject of the post, the non-COVID excess deaths queer up the usual epidemiological tool for gauging epidemics: we are seeing excess deaths even whilst the contribution of COVID is trivial (dark blue on the chart), and when we know that many or most of those COVID deaths are due to false positive tests, and so should be in the cyan section. So we will have no decent tools for assessing this winter’s toll, apart from the kinds of deep dives into statistics by those like John Dee or Professor Fenton.
And so in all probability we are set for the worst winter pandemic death toll ever, leading to further lockdowns and the permanent curtailment of our remaining civil liberties – but quite plausibly with COVID having played little or no part in it at all. Isn’t the Science wonderful?
But do you know what the worst thing is? I will explain this in detail to intelligent people, some with science degrees, who will look blank, keep silent, and not bother to read any documentation I give them. But they will be thinking “But the country’s leading scientists…” Or, like my own brother this week, “Well, you’ve been retired for thirteen years.”
There are a few who are interested in evidence – the rest consult oracles.