
And so the unending cycle continues: this time Boris Johnson warns that lockdown continues (probably) because of the Indian variant, thus proving that as long as micro-evolution exists in Coronaviruses, nothing will stop our lives and economy being put on hold by an ignorant and coercive government. There remains no exit strategy.
Some of us were pretty certain, beyond mere pessimism, that some excuse would be found to prevent the in any case ill-defined return of freedom (would it include masks, or not? Would we require identity surveillance, or not?). The Indian variant was not prevented from crossing from India by the stringent travel restrictions which are relatively easy to enforce by borders and oceans, but apparently the leaky sieve of lockdown restrictions that have so far only served to make life hell and give us one of the higher rates of excess death in the world is expected stop it spreading here. Now, if Boris had locked down hard last February… we’d have exactly the same problem now, of course, but don’t expect that kind of logic from SAGE.
And if the illegal immigrant does spread more readily than the last several variants, so what? Have not the vulnerable been fully vaccinated by the Great British NHS Triumph? There is also significant evidence that, as is usual in viruses, the increased transmissibility, if it exists, has come at the expense of virulence.
The fearmongering over this particular strain is built on the decision to puff the recent situation in India. Cynically, perhaps that news cycle was simply preparation for the new panic. We are expected to associate “Indian variant” with bodies propped up on mopeds, streets choked with funeral pyres and so on.
It is true that India has had a wave of infection, and it may be purely coincidence that it coincided with the rollout of vaccination and a consequent decrease in use of prophylactic measures like ivermectin. But you may have noticed how India has dropped out of the headlines now it has served its purpose, and it is worth calling it to mind as the Gompertz curve of the outbreak has now clearly peaked:
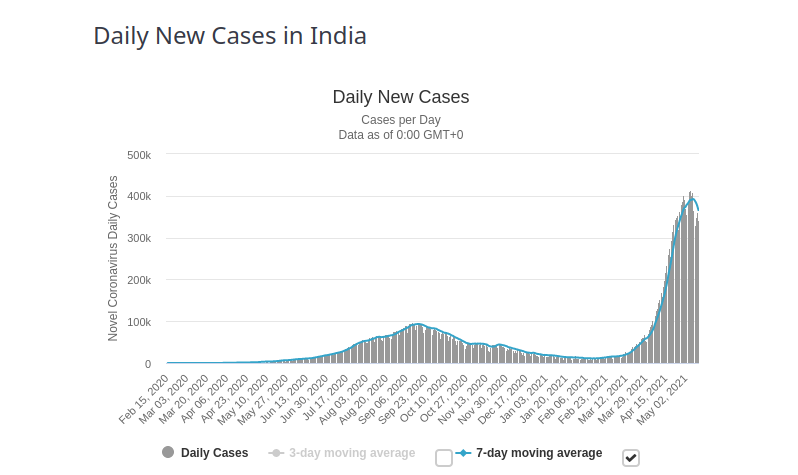
Correspondingly, deaths are likely to be at around their maximum now, at around 4,000 per day. That is a large number in isolation, but one must always remember the denominator, since the official narrative always forgets it. There are 1.1 billion people in India, and this outbreak seems to have affected all regions at the same time (which is odd in itself, but that’s for another discussion).

So let’s compare this Indian wave with the winter outbreak in Britain, which although it shows a double peak, still reflects the universal shape of viral surges:
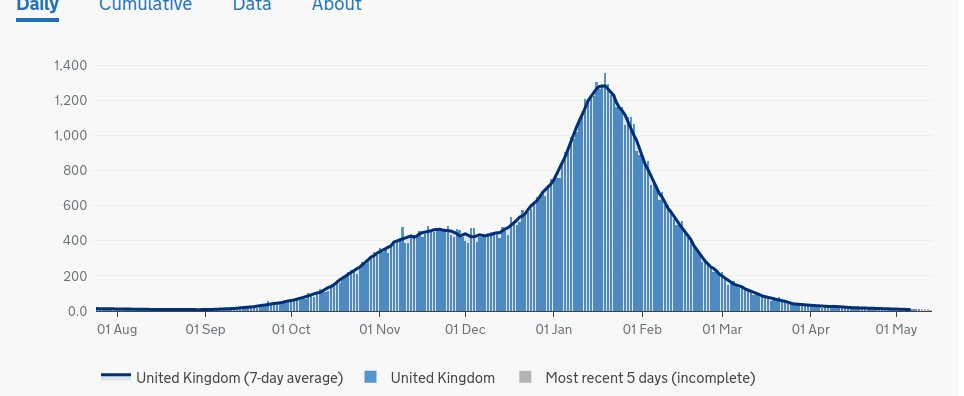
You will see that at its peak we in Britain were getting around 1,500 deaths a day (I am ignoring diagnostic problems both here and in India), though our population is massively smaller that India at around 70 million. A simple calculation shows that the maximum per capita death rate in this Indian outbreak is a mere 1/5 of ours, and looks set to drop from now on. If we had had that rate, it would have meant 300 deaths at the worst stage, and ICUs touting for custom rather than being allegedly close to capacity.
The intelligent question to ask, then, is not whether its strain of COVID will wipe us all out, but just how India has done so well despite a far smaller vaccine rollout, a desperately poor population and (at least in the cities we have been shown) an inadequate and overloaded health service. We ought to be looking to learn lessons from the subcontinent’s policy. That we are not is, I suppose, only to be expected in Bizarro world.
Despite India’s sunshine, it is not because of Vitamin D status, as for various reasons deficiency is very prevalent there. But one part of the answer might be ivermectin use, which has been less successfully suppressed than in many countries including Britain. Ivermectin is in widespread use there as an anti-parasitic on virtually an over-the-counter basis anyway. Some states have been using it routinely in COVID with good results since last year, in conjunction with other agents like budesonide, against the tut-tutting of those areas more open to the influence of the WHO, The Gates Foundation, Big Pharma, and the world political Groupthink that sells the idea that long-established safe treatments are poison.
Nevertheless, a large black market has grown up, particularly among the poor who stand little chance of early vaccination or good hospital treatment. Once this outbreak occurred, the government had a rare attack of virtous panic and authorised ivermectin for use in COVID, as opposed to advanced and democratic Australia where, since April, a doctor can get six months in jail for prescribing it.
There may be other reasons why COVID is on the turn in India, but the fact remains that we suffered five times more daily deaths per capita in the winter than they have now, and whether that is because of their management or because the Indian variant is simply less deadly we ought to be viewing their example as an encouragement, not as yet another means to maintain terror and keep the population in chains.
I’ll close this blog by yet another example of a leading medic, Dr Peter McCulloch, with an interest in treating COVID, not only disagreeing with the mainstream narrative, but discerning a sinister worldwide pattern behind the latter. It’s impossible to look critically at the situation and not conclude that the conspiracy is real eventually.
In this case, it is regarding the total official avoidance of any attempt to organise treatment regimes using the wide range of agents, including ivermectin, now known to be beneficial in multiple trials. When Public Health bodies show no interest in effective treatment – and indeed instead show concerted antagonism, censorship and persecution – but only promote lucrative experimental vaccines, resulting in possibly hundreds of thousands of unnecessary deaths by professional neglect, then they are beyond deserving any vestige of respect. Indeed, “crimes against humanity” is a better description.
A useful well-informed article on the actual state of affairs is here.