
This is an update of things I wrote last summer to remind folks of how a high rate of false positive COVID tests falsifies all the statistics, and not just the case numbers. It’s relevant because SAGE and others are making dire forecasts about the dire effects of repealing our now sketchily-observed restrictions.
First, let me refer you to an astonishing statistical exercise on the ONS data by retired NHS statistician John Dee: see “Viral Testing And Vaccine Fallout” here. Warning: it’s technical.
After crunching the sometimes well-obfuscated official numbers, he comes up with a likely true estimate of the rate of false positive tests at every point of the pandemic. In the quiet summer periods this reaches close to 100% – nearly all of the recent cases, then, have been false, as many of us were saying last summer based on cruder estimates of the PCR false positives then. And why would that not be, since Coronaviruses are strictly seasonal? But Dee does note the slight increase in recent cases, with a corresponding dip in the false positives, in recent weeks, to a mere 93% or so.
He then uses this information, and applies it to the actual numbers of tests done over the course of the pandemic, using the arcane tools of statisticians. You’ll remember that when false positive rates are significant, absolute numbers of positives will be greatly affected by the number of tests done, making the headline figures of “cases” meaningless except to scare people. President Trump was right, not naive, when he pointed out that the more you test, the more disease you’ll find, especially when the test, rather than any symptoms or objective signs, has become the diagnosis in WHO directives. And when there is no effort to make sampling representative – surge testing is guaranteed to skew results in a pessimistic direction.
Dee is astonished to discover that for the whole period since last spring nearly all the variation in case numbers may be accounted for by the variations in test numbers. In practice, the tests (both PCR and LFT) may be performing no better than random number generators.
The best graph to show this in his article is this one:
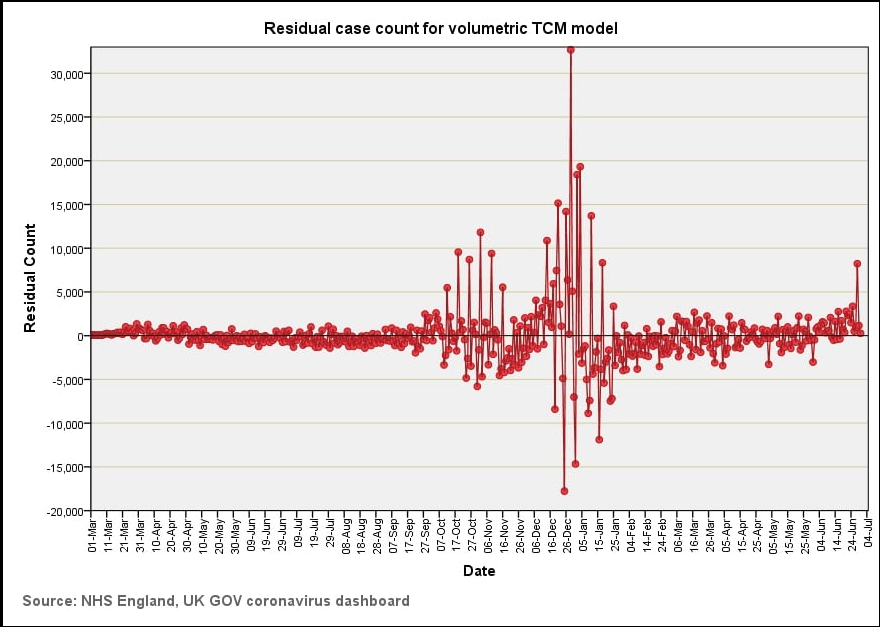
From March to October 2020, compensating for numbers of tests and false positives makes the real cases disappear. He points out that where there then seem to be tall and significant peaks, the data-points (based on daily records) are implausibly varied, strongly suggesting that they have more to do with issues in the collection and publishing of data than with anything significant about the disease. Indeed the only trend he sees is the tendency to a slight rise in real cases since the new year, which he speculates may be due to some untoward effect of the vaccination programme.
That’s the bombshell. My own task here is to remind you how a situation like that must also, eventually, affect the hospitalisation and death statistics and render them meaningless, and this is because of the dubious definitions used for both.
Hospitalisations are defined as any “admission” to an NHS unit (even, for example, a learning disability facility) with a positive test within the previous 14 days or while in hospital. There is no necessary connection whatsoever with COVID symptoms in that definition, and nothing in the available statistics to enable isolation of the real cases from the false positive tests. Note that in-patients are among the most tested groups in the country, and so when COVID incidence is low, as in the summer, their false-positive rate will be particularly high. Worse still, patients tested repeatedly may also be repeatedly added to the numbers.
COVID deaths in the ONS statistics are still defined as any death within 28 days of a positive test. Firstly, then, any patient dying in hospital with a false COVID positive will be counted. But secondly, when tests are at the absurdly high, and steadily increasing level they are at present (1 1/4 million a day) then a small but increasing number of community false positives will happen to die there from common causes. But note that, according to the ONS All Cause Mortality Surveillance our excess deaths are still at an all-time negative rate, and have been since early in the year.
A third measurement, “patients in mechanical ventilation beds” is also slowly increasing, but this is another opaque statistic: ventilators are now seldom used in COVID, so do they mean ICU beds, or are they dragging in those suffering strokes, brain injuries and so on who are on ventilation? Either way, since the country is recording 32,000 positive tests a day, nearly 30,000 of which are likely to be false if Dee’s 93% false positive rate is correct, non-COVID ICU patients will begin to register on the statistics anyway.
But if what I say above is true, the recent drop from the 100% false positive rate that Dee estimates may itself be illusory, because he is factoring in the number of COVID hospitalisations to calculate “real” infections, and we have seen that this figure need not be reliable when testing rates are so high.
What about the peaks at the start of the pandemic, and last winter, then? Dee’s analysis may not speak to the initial outbreak much, because PCR testing was low and, for the only time in the whole period, it was the typical SARS syndrome that overwhelmingly led to diagnosis of COVID illness and death. But his analysis casts doubt on much that was going on last winter, and there are some other interesting features of that peak.
The first is that deaths last winter were only above the common range for a very short period, and according to another analysis of the long-term data by Dee it never rose above the 50-year average (and indeed only did so in early 2020 for a couple of weeks). The second is the almost total disappearance of all the other causes of winter respiratory deaths, such as flu. This could be attributed to mysterious “selective pressure” subduing other bugs, but it might well have more to do with the fact that everybody was tested for COVID at an even higher rate than now (up to 1 1/2 million a day). Nobody was tested for flu – or if they were, it would be COVID that was the cause of death in the records, because clinicians were directed to record even a suspicion as a case.
When there is a high false positive rate, a high testing rate, and a high death rate from winter infections (or any other cause), then there will also inevitably be a high “COVID death rate,” but how much that corresponds to genuine COVID death rates is a moot point. In other words, a pure “casedemic” could show the kind of pattern we saw even last winter, and at the very least, COVID deaths might have been orders of magnitude lower than they seemed, simply increasing what, in its effects, was “a moderately bad flu season.” COVID does seem to have caused real issues last spring, so I suppose it must have caused some deaths last winter. But we have remarkably little to assess it, without John Dee’s painstaking statistical analysis. Wouldn’t life have been so much easier if SARS-CoV-2 infection was treated like a normal disease, diagnosed on genuine clinical criteria and attributed according to Koch’s postulates and so on, as we used to be taught at medical school? But as I have said before, science died last year, and it did not kill itself.
Looking into the future, the media crystal ball again warns us to give the client’s money back. Thus in the Guardian Prof Jon Deeks warns that if daily cases rise to 100,000, 660,000 “gold standard” [sic] PCR tests will be needed every day. On the analysis above, it’s more a case of the reverse: if PCR tests rise to 660,000/day, cases will inevitably rise to 100,000, and probably far more.
There is no realistic likelihood, apart from excess testing, for cases to rise that high. But if they did it would be because SARS-CoV-2 is absolutely everywhere where there are people. So what exactly do they hope to gain from testing anyway?
Ah – I see that John Dee has actually addressed the very issues I raise above regarding mechanical ventilator beds in a new post. Follow link in OP and look for Mechanical Ventilation Bed Use. Depressingly, all the deceptions I name are there, plus a few more he’s heard about from insiders.
After I wrote this, my wife informs me that BBC radio says there is more respiratory disease around than you would expect at this time of year. Have a look at Dee’s chart at “Mechanical Ventilation Bed Use.” This confirms the fact, but denies any of it is due to COVID.
Meanwhile total deaths, as I said in the OP, are below normal.
So what is going on? Do you remember that Dee was questioning the role of the vaccine roll-out?
Jon,
It takes me a few reads of all the technicals to get over my stat-induced vertigo.
Really, one has to be a statistician, a biologist, immunologist, and a doctor in order to have a right to any opinion on all this. Or, that is the way the narrative is sold anyway. It is easy to question the motives of all sides in the Covid story. When I find myself wondering at the motives of people like Robert Malone or Bret Weinstein, I remember who it is that took away our freedoms.
If only people will stop taking the tests. That would put a kink in their corporate covid industrial complex. Until the next scheme.
I appreciate the problem! For myself, I started off knowing something was wrong as soon as they announced lockdowns, and was soon able to see how much of the official story was flying in the face of what i knew as a professional. And that was reinforced by selected reading of various papers.
That apart, I think for the average intelligent person, the principle is “Follow the money.” The guys you can trust are generally the people who have retired, or who have already been fired, or who started out assuming all was well until they started investigating (and there are a lot of those!).