
OK, I refer you to another excellent post by John Dee entitled False Positive Refresher. In it he talks about the PCR test’s sensitivity (which is the nominal percentage of true cases it spots). A sensitivity of 80% means that if you test 100 sick people, it will miss 20 of them. More importantly, in this context, is the specificity (which is the nominal percentage of genuine negatives it spots). So a specificity of 99% means that if you do the test in 100 well people, it labels one as sick, ie as a false positive.
As Dee points out, how much this matters depends on how much disease is actually around. If you do the test with 99% specificity for 99 well people and 1 sick person, you’ll get as many false positives as true positives, which isn’t much use. But, given the 80% sensitivity I used, there’s also a pretty good chance you’ll miss the one sick person and quarantine only a healthy one. And that is truly useless.
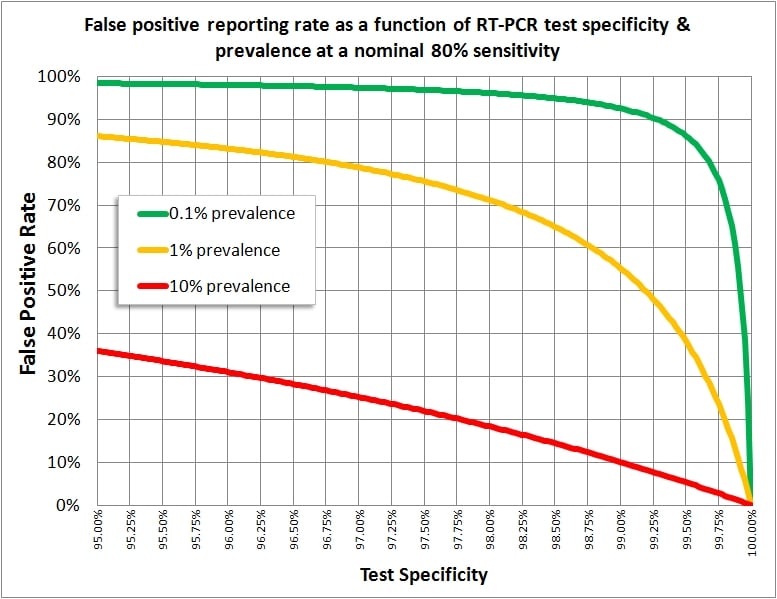
Dee’s chart summarising this is here, and one needs to think about it hard to make intuitive sense of it. The red line shows that, when lots of infection is about (10% of people) even a rubbish test (left end) will give reasonable results – though even then, with a respectable 97% specificity, 25% of your results will be false positives. Still, better to be safe than sorry in a rampant epidemic with bodies in the streets.
But if only 1 in 1000 people is infected in your test population (green line), even a test with almost 100% specificity gives you a false positive rate pushing 100%. Half the world is quarantined – but you’re still only picking up 80% of the few who are actually sick. You’d do as well quarantining alphabetically.
Unfortunately, because PCR, absolutely falsely, is regarded as the gold standard although its true specificity and its sensitivity aren’t even known, we have no way – NO WAY AT ALL – of knowing how much COVID is around at the moment. That’s compounded by the specific problems with PCR of badly controlled “cycle thresholds” and quality control. But there’s every chance that very few of the supposed positives are real, even if we accept what John Dee has been told is a specificity of 99.97% (which seems ridiculously optimistic, and mere guesswork seeing there is no genuine virological standard by which to calibrate it).
So far I’ve just parroted John Dee, badly. But if you understand the argument, which is absolutely sound and basic, you might reply, “But if even a test with a 99.97% specificity rate gives a wildly mistaken impression, what tests can ever be of use to doctors?”
And the answer to that lies at the end of the sentence: “…use to doctors.” Proper doctors do not (or used not to when science existed before last year) go around the country swabbing innocent victims to pin a disease diagnosis on them.
Instead, a patient comes in with a history of symptoms suggestive of a particular condition (or perhaps a few alternative conditions – nature doesn’t make a doctor’s life that easy). Clinical examination will usually provide signs that narrow the possibilities down. And a good diagnostician will usually, when the condition is not a rarity, already have a good idea of what’s going on at that point. Any tests done will be to confirm the diagnosis, and to exclude others.
What that means in relation to Dee’s article and chart is that, in real medicine, the “prevalence” of a disease in the population actually being tested is pretty high, because a skilled clinician has already diagnosed it in all of the people he sends for tests. In a lot of conditions the doctor may have the correct diagnosis 80% of the time or more, which gives an 80%+ prevalence – 8 times better than the best red line on the chart, and therefore producing a line well below the red line.
That means that even a fairly unreliable test will not give a significant false positive rate – and if it does give a dubious result, the clinician will disregard it, use some other test, repeat it – or wait to see how the condition goes.
This is why screening programmes are few, highly structured, and even so are often contested on cost-benefit issues. For example the use of mammography in breast-screening is still on a knife edge between life-saving and worthless, and has been since I was at medical school in 1976.
BUT… governments worldwide, and especially and royally in Britain, have ignored all these basic scientific and medical facts and have forged ahead with mindless screening of whatever moves (or sometimes doesn’t because the patient has already died). Think what this means on the ground, if we accept, for now, that very many COVID tests are going to return false positives. It’s more than just individual misdiagnosis.
In 2019, a patient with the very common symptoms of mild diarrhoea and malaise was probably going to sit it out at home. The few getting to the doctor were going to be diagnosed as suffering from one of many viruses, or under certain circumstances might get stool samples done for food poisoning. My guesstimate is that symptoms suggestive enough to get tested for bacterial poisoning are confirmed bacteriologically maybe 50% of the time. It’s a lot lower when the test is done for occupational reasons rather than on clinical grounds.
Diarrhoea was not initially a COVID symptom, although I’ve no quarrel with its being one of its possible symptoms because it’s a coronavirus, and the spike protein also hits all manner of systems. So the guy on the ventilator with typical SARS, and the squits, might help the latter symptom to be added to the “clinical features” list of COVID – but it’s no more a useful diagnostic feature than “runny nose” is of both a cold and a spinal fluid leak (I see they added the latter to the diagnostic list anyway, so your hay fever may earn you a PCR test now).
But now, everybody who gets abit of diarrhoea after work is immediately tested for COVID, and the usual high proportion come back as false positives. Lo and behold, after a few weeks of reporting this, diarrhoea alone becomes the sole symptom in some cases of COVID (in 2% of cases, as it happens). But a COVID case is defined as someone with a positive test, so the same is going to be true of any symptom you care to name that isn’t arbitrarily ruled out of court (how do you know your athlete’s foot or your appendicitis wasn’t caused by COVID? Because nobody was stupid enough to test you, that’s why).
The limiting case is, of course, the person who has nothing wrong with them at all and gets tested because school or work requires it or they like the idea of free tests. Their numbers will similarly build up until the commonest symptomatology of COVID is being healthy – and Voila! A casedemic. “Freedom Day” becomes, to the prisoner’s dismay, transfer from Belmarsh to an open prison on the basis of an epidemic of wellness, the defining symptom of the deadliest disease not to kill most people.
But the point I have made is independent of the COVID phenomenon itself – there is no test in the world that is reliable enough to be employed as the sole means of diagnosis when screening entire populations. Tests should only be used by doctors who can make halfway-decent diagnoses without them. And the government scientists who ever recommended the idea prove themselves to be complete charlatans or evil conspirators, because it’s yet another example of the bleedin’ obvious.