
I, and others, have long been pointing out that, quite apart from the intrinsic specificity (false positive) rate of the PCR tests it has been very difficult to get hold of details on how many amplification cycles are being used in real life. The original British standard was 45 cycles (to be “on the safe side” over the WHO’s recommended 40 back last year).
In case you’re not up to speed on this, the WHO’s definition of a COVID-19 infection is one positive PCR test, there being no firm clinical criteria or a virological assay. PCR is considered the”gold standard” of diagnosis because there is no gold standard. It is the diagnostician who can never be mistaken by definition, but slaps the same diagnosis on everyone he meets. This makes the test enormously vulnerable when being used for screening well people.
At various stages the government has put out guidelines saying that only symptomatic people should be tested, and then has totally ignored them in rolling out mass testing. There is also a document that made recommendations about the maximum cycle threshold to avoid false positives. I’ve forgotten the actual value, but the big question has been whether labs across the nation have taken these guidelines on board.
It matters, because even Dr Fauci has said that above about 25 cycles, a positive result is extremely unlikely to represent an active infection. Therefore no test above that kind of range is of any diagnostic significance. The inventor of the test, the late Kari Mullis (who got a Nobel Prize for it) said it should not be a clinical diagnostic test, stating publicly that it would identify any molecular fragment in any person with enough amplification cycles. Here’s the problem:
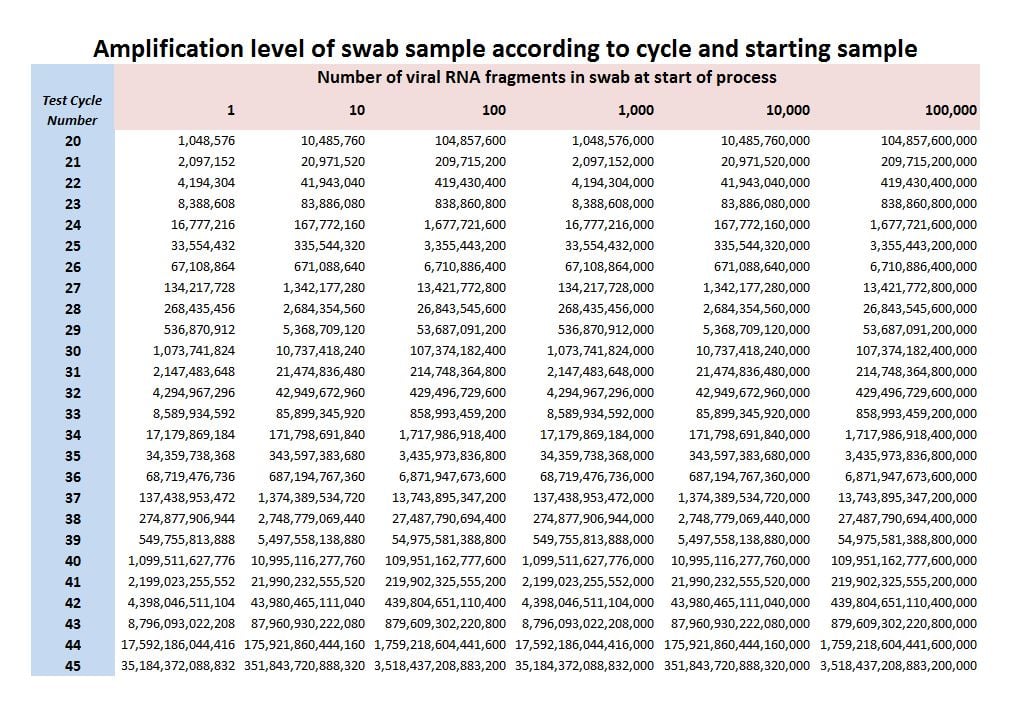
Each cycle doubled whatever is in the sample, rather like the old story about the emperor paying for services with doubling grains of rice on a chessboard. His empire was bankrupt long before 2^64 grains (that’s 64 cycles in PCR money). You’ll see from the chart that, at the old UK recommended 45 cycle threshold, even 1 viral RNA fragment will produce 35 trillion copies. Quite apart from left over fragments from infections, or minimal circulating virus in the immune, the possibility of minimal lab contamination will generate a positive.
That means that the vast majority of “gold standard” tests are bound to be false positives unless you happen to be testing a ward full of SARS patients.
Well, some public-spirited soul has thought to make an FOI request from Manchester University NHS Trust – which one would assume to be a lot more reliable than some private company’s car-park test centre:
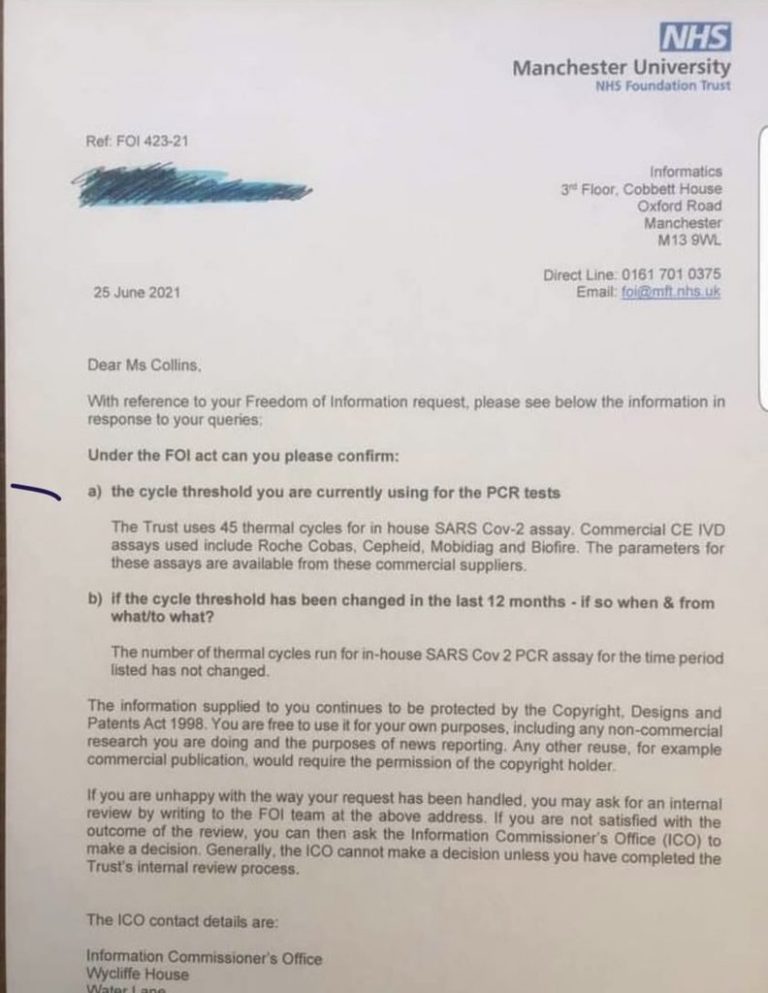
And as you see, no message about reducing the cycle threshold has ever been sent to, or received by, them. They’re still doing 45 cycles, and generating epidemiological white noise rather than test results. No wonder John Dee found no correlation whatsoever between adjusted test results and hospital COVID activity.
Now, since deaths are flatlining, and hospitalisations, for what the figures are worth diagnostically, rising but far below winter levels, the entire cancellation of the actual benefits of Freedom Day on Monday, with all the venues scared into requiring proof of vaccination or negative tests, masks and social distancing, are based on nothing more than a piss-poor national test regime.
But we knew that already, I guess.
Just looking at the table above, to give some idea of the nonsense – at the “legit” threshold of 25 cycles, 100,000 virus particles will magnify up to around 3 trillion, and you’ll get a nice strong positive that’s reliable.
At the UK’s 45 cycles, just 1 moth-eaten scrap of possible virus will give you ten times as many particles – 35 trillion – and the “positive” needle will be off the scale.