
We had an excellent pub lunch on our daughter’s birthday yesterday. A lovely warm and cosy thatched village hostelry, with a log fire. It was obviously very popular because every table was full. We spent a couple of hours there over an excellent meal and their home-brewed bitter. And the only masks in sight were on a few of the newcomers sporting their cosmetically-compliant face-rags as they came through the deserted lobby to the sparsely-occupied bar, before being ushered to their convivially-packed tables and removing the masks.
In other words, barring the cleansing updraft from the fire, it was an ideal environment for viral aerosols to hover, should one be worried about a virus that is now endemic and, in its new Omigosh variant, appears to be reducing hospitalizations and deaths rather than increasing them. “Cases” are going up, but only in line with increased testing.
Our village COVID incubator is, of course, entirely legal. But in case those living abroad aren’t up to date (and those in Scotland and Wales haven’t noticed) the government’s panic response to the variant has been to make masks mandatory in shops and public transport. This is entirely typical of the incoherence of our public health policies: virtually no outbreaks have ever arisen in shops (and precious few in pubs, actually – homes and hospitals are the death-traps), which is scarcely news as many staff have worked in supermarkets unmasked for most of the pandemic and have stayed healthy.
I know that half an hour pushing a trolley around an air-conditioned, high ceilinged and uncrowded Tesco makes me much less exposed to aerosols than two hours in our cosy village pub did. And so do the authorities, but they have chosen to regulate the former and leave the latter alone, for now, for reasons entirely opaque. Perhaps the sacred oracle decreed it thus. But thank the Lord anyway for small mercies. No doubt it will all change for the worse when increased testing forces the case-rate up and some of them happen to be Omigosh, even if the hospitals and mortuaries are empty. Experience shows that governments like to put up legal barriers to keep COVID out of places where it is already common. Being obsessed with rules seems to make one blind to logic, but hypersensitive to non-conformity.
Let me give you another example. In March, a COVID outbreak swept through a care home in the seaside town of Sidmouth, not far from us. Eleven elderly people died. But the odd thing was that they had all received their first dose of vaccination a few days beforehand. In fact, it wasn’t odd at all – I, like others, had already been aware of the phenomenon of outbreaks in recently vaccinated care-homes, and although it was not enough of a trend to be incontrovertible (as it is now, through worldwide instances) my first impression was, “So it’s happening here, too” rather than “That’s impossible.”
If you search the old news reports now, apart from the increasing death count from day to day, what is most obvious is the progress of the police investigation into suspected neglect. This resulted in two care-workers being charged and bailed, but eventually not prosecuted because of insufficient evidence. It took until June for the sword of justice to be removed from their necks, however. They were charged because the police could not believe that such a tragedy could result from anything other than someone breaking the rules.
On reflection the tragedy is far more likely to have been the result of keeping the rules by sticking AstraZeneca into the arms of a demographic in whom it had not been tested, within a population in whom it had not been tested adequately (in trials, from all appearances, in which any patients showing problems immediately after vaccination were simply excluded from the trials, and so not counted).
So there should indeed have been an investigation, but not a police investigation – or at least not until the sharp practices of the Pharma corporations were brought to light. It should have been, and in any rational country it would have been, a scientific investigation into what made recently vaccinated geriatrics particularly susceptible to COVID. Unfortunately there seems to be no rational country left, or no doubt its beaches would be full of dinghies bearing refugees from former western democracies
An article by HART offers the possible explanation that SARS-CoV-2 is often latent or dormant in asymptomatic people. This is true for other viruses, probably explaining the outbreak of colds several months into tours of duty at antarctic stations. The triggering of shingles (the reactivation of old chickenpox viruses in the nerve ganglia) by COVID vaccination shows that they can indeed reactivate dormant virus infections. It is quite possible, then, that something good in that care home’s regime had kept the old folks healthy despite their contracting the virus, until vaccination suppressed their immunity and killed them. If there was such a protective regime, it was punished by police charges and bail.
Certainly the police were unable to find any alternative explanation in the breaching of rules. But nobody thought to investigate the possibility that inadvertent medical mismanagement caused their deaths, by investigating either the dead or the survivors. The former were all cremated without post-mortems (COVID is too dangerous for coroners, you see), and no doubt the latter were banged up in isolation for the rest of lockdown like so many other poor souls. The doctors are all too busy with the booster merry-go-round to do research on adverse reactions.
But the HART article suggests this might be rather important. Here is a chart from the article comparing UK COVID death rates with those of Europe as a whole:
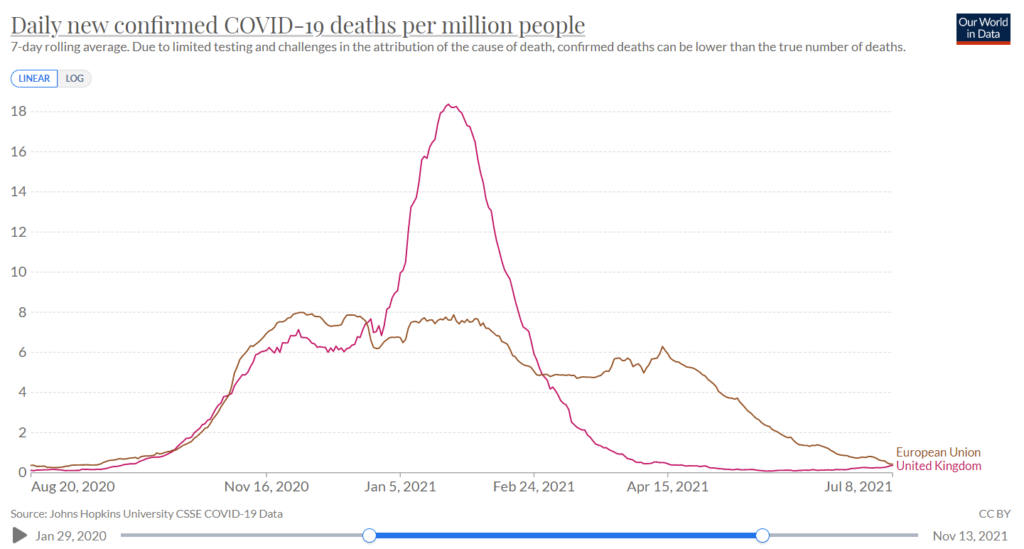
Now it is just one chart, and so is fraught with possible confounding factors. We’ve often discussed the meaninglessness of the UK “deaths within 28 days of positive PCR” definition, and each country in Europe has its own unique and dubious standards.
The link with vaccination rates, too, is potentially murky. But it is a fact that Britain was unusually quick off the mark with its own vaccine, AstraZeneca, and for once (to our credit) rolled it out in an orderly manner starting with the most vulnerable. European countries, by contrast, faffed around without a coordinated policy, acted late, injected across the population more sporadically, and varied greatly in a generally slow roll-out.
So it may be fair to say that the sharp UK peak of deaths in February corresponds to the peak of our vaccine roll-out, and a temporary loss of immunity following, to those likely to die from COVID. This peak is lacking in Europe apart from a wider and lower peak centred on April, an unlikely time for a seasonal COVID outbreak. HART’s suggestion is that the area under the graph (corresponding to the total deaths/million), which is equal, might mean that the vaccines don’t actually work, but simply kill the vulnerable earlier. It is worth considering. It would, of course, need more sophisticated comparisons to confirm.
But as I have been pointing out, governments, government scientists and health services seem more committed, currently, to imposing worthless rules, and enforcing them with draconian penalties, than with any kind of scientific assessment of public health policy. They are sold on vaccines at all costs, vaccine passports, vaccine mandates, and vaccine concentration camps. Because vaccines are safe and effective, by definition it seems, even if they have so far killed nearly 33,000 people across Europe according to EudraVigilance (but what price vigilance if the garrison ignores the trumpet?)
That policy is a very bad thing, except in that, at the moment, it discourages me from walking around Tesco, but encourages me to sit in a warm pub with friends and family, and spread the word about the current insanity.