
When I was a GP the drug companies blanket-advertised the wondrous benefits of statins for increasingly normal patients. The NHS guidelines, sadly ultimately under the thumb of Big Pharma, followed suit in incentivising us, with both carrots and sticks, to prescribe them to ever increasing numbers of people with marginal risk factors discovered at increasingly mandated routine checks.
I found back then that the most useful way to inform patients of the actual risks and benefits to them was to go behind the apparently massive percentage reductions in heart attacks from statins, and work out the “NNT” (number needed to treat) from the incidence of the condition and the risk calculators. If a patient was told that 150 patients like him would need to be on lifelong statins to prevent one heart attack (and even fewer deaths), that is that 149 people would be taking them unnecessarily, their personal risk calculus was, quite rightly, often adjusted by the patients.
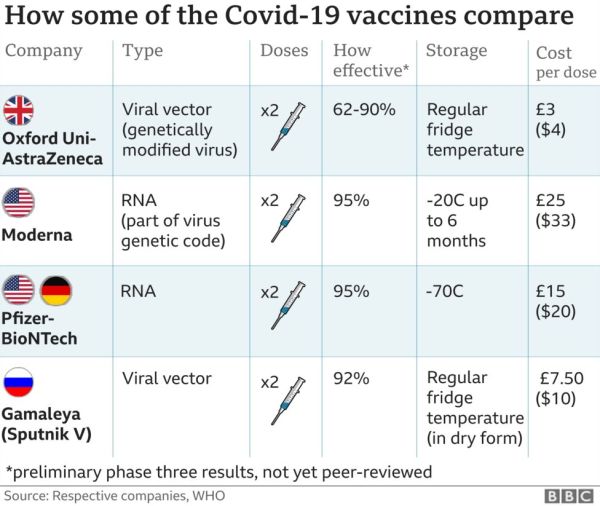
The same situation obtains regarding COVID vaccination, which has been ruthlessly pursued as the only possible solution to the disease using the kind of “95% reduction in cases” findings of the original trials and the FDA’s briefing documents. Here’s an example of the kind of upbeat chart that we were all shown to encourage us to get the shot:
But these high percentages are calculated from, for illustration, two people out of 2,000 in the trial getting COVID without the vaccine, and only one with it, which a 100% relative reduction. But it has already been pointed out by doctors that using these “relative reduction rates” gives a poor indication of the actual individual and societal benefit of an intervention, which is why in every case except, inexplicably, these vaccines “absolute reduction rates” are mandated in trial reports as well. And so, in my fictional example, one less person in 2,000 got the disease, which is a tiny benefit for an awful lot of vaccinations.
Now, a Lancet article by Piero Olliaro, Els Torreele and Michel Vaillant crunches the numbers from the original trials to correct this omission, and most usefully includes the “NNT.”
The results appear in a pdf appended to the paper, but a suitably polemicised and simplified version is this:
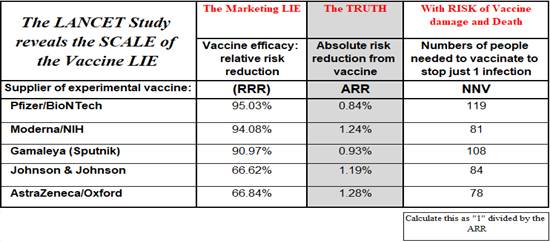
You will see that for all the vaccines, the number of folk needing to be vaccinated to prevent one COVID case hovers round the 100 mark. And that doesn’t sound all that brilliant, especially given that the trials were done when COVID had a relatively high incidence in the trial populations, whereas in the current northern hemisphere summer the virus has almost disappeared. That NNT would be far higher if based on current data.
One must also bear in mind that the vaccine trials had a very low threshold for recognising a COVID case, usually doing a PCR, with unspecified amplification cycle criteria, in the presence of the merest sniffle. The number of actual COVID infections was therefore undoubtedly lower than stated, both in the vaccinated and un-vaccinated groups
But the real shocker is to extrapolate the conclusions of this paper to the known Infection Fatality Rate of COVID, which is (worldwide) around 0.15%, or 1 in 750 actual cases, based on serology. This figure comes from the worldwide study by John Ioannidis cited by the WHO itself – though remarkably unnoticed by the press.
On that basis, the NNT to prevent just one COVID death will be in the order of 75,000. One would have to question the value of mass vaccination for that outcome, even if the vaccines were known to be 100% safe rather than being in an uncontrolled Phase 3 trial with increasing reports of fatalities. As the Lancet article reminds us:
Uncoordinated phase 3 trials do not satisfy public health requirements; platform trials designed to address public health relevant questions with a common protocol will allow decisions to be made, informed by common criteria and uniform assessment. These considerations on efficacy and effectiveness are based on studies measuring prevention of mild to moderate COVID-19 infection; they were not designed to conclude on prevention of hospitalisation, severe disease, or death, or on prevention of infection and transmission potential. Assessing the suitability of vaccines must consider all indicators, and involve safety, deployability, availability, and costs.
But the phase 3 “trials” of these vaccines are actually just an untidy mass roll-out, with all efforts being made to maximise the take-up by minimising the recognition of adverse effects, so that estimating the fatalities is more than usually difficult.

So far something over 1,000 UK yellow cards for deaths possibly linked to vaccinations have been returned by doctors or members of the public. On the one hand, the MSM “fact checkers” point out that these reports are not confirmed vaccine deaths. On the other hand, our yellow card system is the main way that adverse reactions may be spotted in new products in Britain, and it is also the case that only a minority of problems ever get reported by the system before they begin to be recognised (as I know, having used it for my whole career). It took over a year for the narcolepsy complications of the GSK vaccine Pandemrix to be recognised in the 2009 swine flu pseudo-pandemic. Before then, isolated cases were assumed to be coincidences, and therefore seldom reported.
So, duly noting the likely inaccuracies, 1,000 suspicious deaths are now reported among some 35 million people who have received the first vaccine dose – a nominal fatality rate of 1 in 35,000. On the face of it the number killed appears to be around double the number saved by the vaccines. As they say in the scientific papers, “further research is urgently required.”
This is even more the case because those still to be vaccinated are the groups at little to no risk of death from COVID. We all knew even in March 2020 that the disease is massively biased towards harming the elderly, so that in their case the risk/benefit calculus is possibly far more favourable towards vaccination – provided, of course, that even the elderly are properly informed that there is a real risk, rather than being blithely assured that “vaccines are safe” or that “the benefits far outweigh the risks.”
In the case of the younger adults, the pregnant women and the children, though, those assurances are almost certainly nothing short of an outright lie. There are virtually no risks of death, or even serious illness, from the infection in these groups in the absence of other serious disease. But there are increasingly well established risks from the vaccines, which risks some suggest to be even greater in the young (though that might be partly because adverse effects like heart problems and strokes are more noticeable amongst the young).
Note that the apparently scientific conclusions reached in the Lancet article actually stem from the original misleading reporting of the trial data, responsibility for which lies at the door of the pharmaceutical corporations, or the government health agencies sponsored by them, or both.
Remember that this vaccination campaign has occurred against a background of the deliberate and concerted suppression of information on cheap and effective therapeutic solutions to prevent and treat COVID (with little or no risk, far lower costs, and massively smaller NNTs), as discussed, for example, by Brett Weinstein and Heather Heying here, or more polemically but equally authoritatively, by former Pfizer research vice-president Dr Mike Yeadon here… or at least it was there until YouTube censored him.
One clear motive for this suppression is that the emergency authorisation of these vaccines, at least in the US, was entirely dependent on the absence of alternative treatments. If ivermectin or other agents are allowed to be recognised as effective, the vaccines must be withdrawn, and both the gravy-train of endless Pharma profit, and whatever ideological agenda underlies the international elite’s obsession with vaccinating everyone for everything, would be destroyed. And so instead the ethical doctors and the innocent public must be sacrificed. There is no other plausible or benign explanation for such fanatical censorship, including threats to strike off or even imprison doctors (Australia) if they prescribe such drugs.
The Lancet article has also been published in a country whose government has within the last week or so used its emergency powers, rather quietly, to slip through legislation allowing sole consent for medical procedures to be given by thirteen year olds. The fact that the US passed similar legislation, equally quietly, on the very same day is, of course, one of many pure coincidences during this pandemic. Perhaps the laws were passed simply to allow children to undergo gender transition against their parents wishes, rather than so they can be pressured or propagandised to be vaccinated at school without parental consent – in which case, of course, the legislation is entirely innocent [irony].
At the risk of tiring you, it is also in the context of insignificant variants, which show no sign of even causing serious illness, let alone death, being bigged-up by the government to blackmail the cautious or well-informed members of the population into getting vaccinated, or being deemed the “selfish” scapegoats for lockdown continuing after June 21st, as hinted by Boris Johnson when he’s not hinting the opposite.
Bottom line: it is clear that for a variety of commercial, political and ideological reasons Big Pharma, governments and government scientists, the WHO, social media platforms and the various other hangers-on going through their revolving doors are more than heavily invested in vaccinating the world whatever the cost. It is also clear that the human risks of such a plan are very low in their priorities, so that as far as staying alive is concerned, it’s a question of “every man for himself” rather than following the programme.
And that is a shame, given our reasonable expectation of being democratically governed for our own good.
Talking of irony: if in the UK they are talking up variants to push people to get vaccinated, elsewhere they’re restricting travel to the UK because they say that “there is no guarantee” that the vaccine will defend against them!
Even though the recent news is that (as expected, and like all the others) the vaccine works fine against it. And in any case all the variants appear everywhere if you wait a week or two – I wonder if there’s a single example of restrictions keeping any of them out, apart from Fortress NZ etc. And if they do keep them, are they cutting off the world forever?
A bit of an update on the above, on the basis of the latest yellow card figure:
A little more optimistic, but still suggested that the number of vaccinations needed to prevent one death is rather the more than the number need to kill one innocent bystander. Not especially good therapeutics, it seems to me.